Abstract
Waiting has become a defining feature of Canada’s healthcare system. This system, founded on principles of accessibility and universality under the Canada Health Act, continues to face a critical challenge: long wait times for essential medical services. In 2024, the median wait time for healthcare treatment in Canada rose to 30 weeks—a substantial 222% increase since 1993 (Moir and Barua, 2024). Over 17,000 Canadians have died while waiting for surgeries or diagnostic scans, exposing the fatal consequences of delayed care (Craig, 2024). This essay critically examines how systemic inefficiencies compromise equitable access and undermine the foundational values of Canada’s healthcare system. Furthermore, it explores how Canada arrived at this crisis and outlines strategies for reform. Through nationwide adoption of centralized booking systems, modernized physician compensation models, AI-driven resource optimization, and strategic reinvestment in both primary and specialist care, Canada can reaffirm its healthcare promises and address the mounting wait-time crisis.
Evolution of Public Policy for Healthcare Accessibility
Accessible healthcare is essential for a fair and equitable society. The Canada Health Act claims to embody this principle, mandating that provincial healthcare systems provide reasonable access to medically necessary services. Yet for many Canadians, “reasonable access” remains an unkept promise. Reports reveal unacceptably long delays in accessing specialists, diagnostic tools, and surgical interventions (Craig, 2024; Moir and Barua, 2024). These issues are exacerbated by uneven resource distribution, greater patient volumes, and outdated systems. The purpose of this essay is to outline these challenges and propose actionable solutions to realign Canada’s healthcare system with its founding principles.
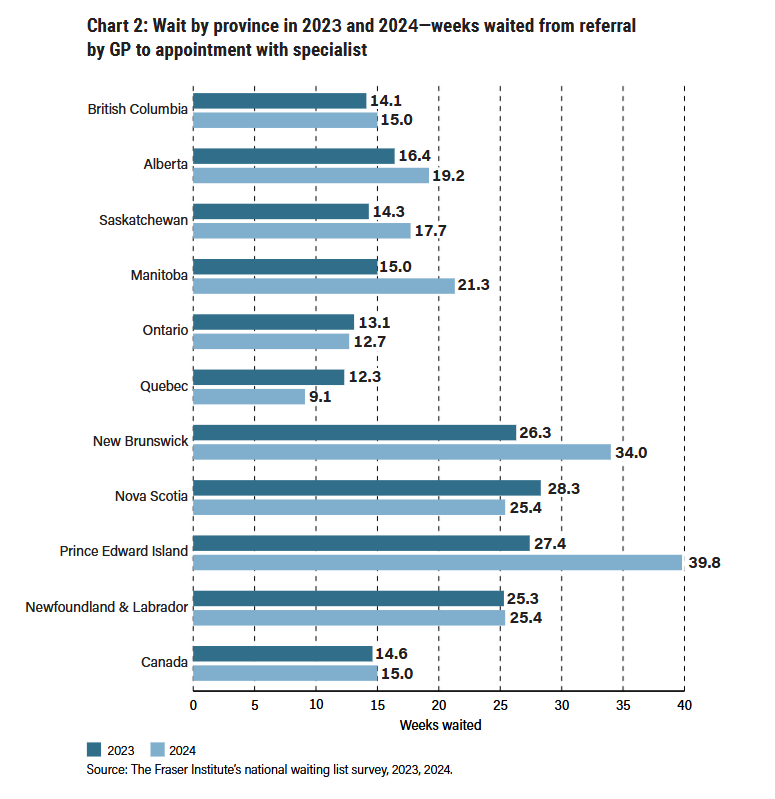
The Canada Health Act’s origins lie in Justice Emmett Hall’s Royal Commission on Health Services, which emphasized accessibility and universality as guiding tenets of Canadian healthcare (Hall, 1964). Yet, the system has struggled to uphold these values. Between 1993 and 2024, median wait times, from referral by a general practitioner to specialist appointments, rose from 3.7 to 15 weeks (Moir and Barua, 2024). Furthermore, an analysis of 11.2 million emergency department (ED) visits in Canada revealed that ED wait times are 17% higher than 5 years ago, with 29% of Canadians waiting over 4 hours to see a physician (McIntyre and Chow, 2020).
Geographic disparities only add to the problem: patients in Prince Edward Island endure median waits of 77.4 weeks, compared to 23.6 weeks in Ontario (Appendix Chart 1) (Moir and Barua, 2024). Such contrasts reveal a fractured system where accessibility depends largely on location rather than need.
The Impact of COVID-19
The COVID-19 pandemic placed unprecedented strain on Canada’s healthcare system. Hospitals faced overwhelming patient volumes, elective surgeries were postponed, and staff shortages reached critical levels (Breton et al., 2022). However, the crisis also served as a catalyst for innovation.
Quebec and Nova Scotia introduced centralized booking systems to streamline patient navigation and reduce wait times for unattached patients (Breton et al., 2022). These systems demonstrated promise by improving scheduling efficiency and ensuring more equitable access to specialists (Breton et al., 2022). However, their uneven implementation across provinces highlights the need for a standardized, nationwide approach. Without a coordinated effort, these isolated improvements risk being inconsequential.
Telemedicine also emerged as a vital tool during the pandemic, expanding access to primary care, particularly for those in rural and remote areas (Breton et al., 2022). However, its long-term integration faces hurdles such as regulatory barriers, inconsistent reimbursement models, and digital accessibility for marginalized populations.
The Cost of Delayed Care
The consequences of prolonged wait times are devastating. In 2023 alone, over 17,000 Canadians lost their lives waiting for surgeries or diagnostic procedures (Craig, 2024). Laura Hillier’s story—an 18-year-old leukemia patient who died after a seven-month wait for a bone marrow transplant—represents the tragic human cost of these delays (Craig, 2024). Her death emphasizes how systemic inefficiencies can have fatal outcomes.
Beyond mortality, the economic toll is also significant, as patients face lost productivity and out-of-pocket costs while awaiting care. In Canada, it has been estimated that the cost of waiting per patient was approximately $2871 in 2023 (Moir and Barua, 2024). Rural and Indigenous populations bear a disproportionate share of this burden, often traveling hundreds of kilometers for specialist services (Karunanayake et al., 2015; Yangzom et al., 2023). These inequities expose a system failing its most vulnerable.
Underlying Systemic Issues
Several systemic concerns underlie Canada’s wait-time crisis. Workforce shortages and infrastructure deficits are perhaps the most significant. In 2024, over 1.5 million procedures were delayed due to insufficient resources (Moir and Barua, 2024). Rural and remote areas face unique challenges, including limited access to specialists and diagnostic facilities (Karunanayake et al., 2015). Geographic disparities in care availability leave many patients stranded, particularly those without the means to travel.
Fragmentation within provincial healthcare systems further complicates the issue. Without integrated referral systems, unattached patients—those without a dedicated primary care provider—often face prolonged delays (Breton et al., 2022). The lack of a national patient database results in redundant testing, miscommunication between providers, and inefficiencies that worsen access problems.
Future Directions and Innovative Solutions
Addressing Canada’s growing wait-time crisis requires a combination of innovative yet pragmatic solutions that balance feasibility with potential for change. Decentralized care models, such as community-based triage centers and mobile clinics, could alleviate pressure on hospitals, particularly for geographically isolated, rural areas (Grady et al., 2023; Karunanayake et al., 2015). Expanding physician compensation models like Ontario’s Family Health Teams, which combine salary-based and capitation models, may enhance patient access (Grady et al., 2023). These alternative pay structures work by incentivizing preventative care through fixed rates instead of traditional fee-for service models that encourage healthcare providers to perform more services (Grady et al., 2023; Newton, 2023).
Another approach to bolstering Canada’s healthcare system is enhanced recruitment of international medical graduates and streamlining their accreditation processes, removing unnecessary barriers that deter potential physicians (Neiterman et al., 2017). Of course, it is still pertinent that a standard of competency is assessed when recruiting international graduates, similar to domestic students. However, unnecessary barriers for these graduates only corrode Canada’s healthcare system even further, when what is desperately needed is an infusion of physicians.
Furthermore, coupling decentralized care models with nationwide implementation of centralized booking systems is another logical approach. These systems have already proven effective in provinces like Quebec and Nova Scotia, where they streamlined referrals and reduced delays for unattached patients (Breton et al., 2022). Expanding this model across Canada would standardize access and alleviate domestic system pressures.
Given rapid changes in the technology sector, artificial intelligence (AI) holds transformative potential for optimizing healthcare delivery. AI-driven triage systems can prioritize urgent cases and improve care pathways. For example, AI applications in radiology have already reduced imaging backlogs by enhancing diagnostic accuracy (Najjar, 2023). However, implementing such technologies requires careful validation and robust methods for data management (Government of Canada, 2025; Najjar, 2023; Pinsky, 2024).
Despite the potential behind these structural changes, these solutions face major implementation barriers. Since healthcare is a provincial responsibility in Canada, national standardization of AI-driven triage systems or centralized booking platforms becomes complicated (Government of Canada, 2025). Moreover, data privacy concerns and Canada’s strict regulations on personal information protection, such as PIPEDA, pose obstacles to nationwide health data integration (Sarabdeen et al., 2022). Even workforce changes remain uncertain, as physician associations may resist shifts in compensation structures, while rural recruitment challenges continue to persist (Karunanayake et al., 2015; Newton, 2023). Thus, while these strategies offer promising approaches for reducing wait times, their success depends on phased, evidence-based implementation to navigate Canada’s healthcare constraints.
Lessons from International Models
Canada can draw valuable insights from successful international healthcare systems to address its challenges with wait times and access to care. The Netherlands, Switzerland, and the European Union offer particularly compelling examples of how policy innovations can enhance healthcare efficiency and equity.
The Netherlands’ healthcare system employs an Activity-Based Funding (ABF) framework, which ties funding to service volumes. This model incentivizes hospitals to optimize their processes and reduce wait times without compromising care quality (Palmer et al., 2013). For example, elective surgery wait times in the Netherlands have been reduced to an average of 1.5 months – a stark contrast from Canada’s 30-week median (European Observatory on Health Systems and Policies et al., 2020; McIntyre and Chow, 2020; Palmer et al., 2023). Implementing a similar model in Canada could address delays for high-demand services by linking financial incentives to hospital performance metrics.
Switzerland’s managed competition model successfully integrates public and private healthcare systems, maintaining universal access while reducing system inefficiencies (European Observatory on Health Systems and Policies et al., 2020). Their system ensures coverage through mandatory health insurance, while subsidizing those with lower incomes (European Observatory on Health Systems and Policies et al., 2020). This balance demonstrates that universal healthcare and market principles can coexist to optimize patient care. While complete privatization is politically unachievable in Canada, adopting a mixed model for elective procedures and specialist services could improve efficiency without compromising universal coverage.
Finally, the European Union’s Directive 2011/24/EU on cross-border healthcare enables patients to seek timely medical care in other EU member states while being reimbursed by their home country (European Observatory on Health Systems and Policies et al., 2020). This policy mitigates domestic system pressures and offers patients alternative treatment pathways (European Commission, 2024). Such a framework also ensures that the right to healthcare is upheld across borders, fostering equitable access for all citizens. Adopting a comparable system in Canada, where patients in “high-wait provinces” can readily access care in “lower-wait provinces”, could help alleviate system pressures.
These examples reinforce how strategic reforms, rooted in international best practices, could help Canada enhance the accessibility of its healthcare system while upholding its foundational principle of universality. By adapting these international policies, Canada can implement reforms that improve efficiency and access.Bottom of Form
Conclusion
At its core, the wait-time crisis raises ethical concerns about equity and what can be considered “reasonable access” to healthcare. The Canada Health Act guarantees reasonable access to care, yet prolonged wait times disproportionately impact the most vulnerable—including rural residents and Indigenous communities (Karunanayake et al., 2015; Yangzom et al., 2023). Policymakers must confront the reality that timely access to healthcare is a fundamental human right, not a privilege. Healthcare delays are not just statistics; they are lived experiences of pain, loss, and diminished quality of life. Addressing these barriers is not just a matter of convenience—it is a moral imperative. Policymakers must move beyond reactive measures and commit to proactive, structural reforms that prioritize patient outcomes.
Canada’s healthcare system is fragmented. Prolonged wait times are reducing public trust in a system that was built on principles of accessibility. Through reinvesting in primary care, embracing technological innovations, and learning from international best practices, Canada can reclaim its commitment to timely care. However, these changes require coordinated efforts at federal, provincial, and institutional levels, alongside meaningful collaborations with healthcare providers and community stakeholders. The future of Canada’s healthcare system depends on its ability to transform principles into action—ensuring that no one is left waiting when their health is on the line.
References
Bouwstra, H., Wattel, L. M., de Groot, A. J., Smalbrugge, M., & Hertogh, C. M. (2017). The Influence of Activity-Based Funding on Treatment Intensity and Length of Stay of Geriatric Rehabilitation Patients. Journal of the American Medical Directors Association, 18(6), 549.e15–549.e22. https://doi.org/10.1016/j.jamda.2017.02.003
Breton, M., Marshall, E. G., Deslauriers, V., Smithman, M. A., Moritz, L. R., Buote, R., Morrison, B., Christian, E. K., McKay, M., Stringer, K., Godard-Sebillotte, C., Sourial, N., Laberge, M., MacKenzie, A., Isenor, J. E., Duhoux, A., Ashcroft, R., Mathews, M., Cossette, B., Hudon, C., … Green, M. E. (2022). COVID-19 – an opportunity to improve access to primary care through organizational innovations? A qualitative multiple case study in Quebec and Nova Scotia (Canada). BMC health services research, 22(1), 759. https://doi.org/10.1186/s12913-022-08140-w
Craig, C. (2024, May 8). Waitlist deaths at five-year high. POLICY BRIEF: Died on a Waiting List. https://secondstreet.org/2023/12/06/waitlist-deaths-at-five-year-high/
European Commission. (2024, April 17). Data on cross-border Patient Healthcare following directive 2011/24/EU for reference year 2022 https://health.ec.europa.eu/publications/data-cross-border-patient-healthcare-following-directive-201124eu-reference-year-2022_en
European Observatory on Health Systems and Policies, Marchildon, Gregory P., Allin, Sara & Merkur, Sherry. (2020). Canada: Health system review. Health Systems in Transition, 22 (3), World Health Organization. Regional Office for Europe. https://iris.who.int/handle/10665/33631
Government of Canada. (2025). Consultations on the AI strategy for the federal public service: What we heard. https://www.canada.ca/en/government/system/digital-government/digital-government-innovations/responsible-use-ai/consultations-ai-strategy-federal-public-service-what-we-heard.html
Grady, C., Chan-Nguyen, S., Mathies, D., & Alam, N. (2023). Family physicians partnering for system change: a multiple-case study of Ontario Health Teams in development. BMC health services research, 23(1), 1113. https://doi.org/10.1186/s12913-023-10070-0
Hall, E.M. Royal Commission on Health Services, 1964. Vol I. JAMA. 1964;190(13):1138. doi:10.1001/jama.1964.03070260050026
Karunanayake, C. P., Rennie, D. C., Hagel, L., Lawson, J., Janzen, B., Pickett, W., Dosman, J. A., Pahwa, P., & The Saskatchewan Rural Health Study Group (2015). Access to Specialist Care in Rural Saskatchewan: The Saskatchewan Rural Health Study. Healthcare (Basel, Switzerland), 3(1), 84–99. https://doi.org/10.3390/healthcare3010084
Mackenzie Moir and Bacchus Barua (2024). Waiting Your Turn: Wait Times for Health Care in Canada, 2024 Report. Fraser Institute.
McIntyre, D., & Chow, C. K. (2020). Waiting Time as an Indicator for Health Services Under Strain: A Narrative Review. Inquiry : a journal of medical care organization, provision and financing, 57, 46958020910305. https://doi.org/10.1177/0046958020910305
Najjar R. (2023). Redefining Radiology: A Review of Artificial Intelligence Integration in Medical Imaging. Diagnostics (Basel, Switzerland), 13(17), 2760. https://doi.org/10.3390/diagnostics13172760
Neiterman, E., Bourgeault, I. L., & Covell, C. L. (2017). What Do We Know and Not Know about the Professional Integration of International Medical Graduates (IMGs) in Canada?. Que sait-on et qu’ignore-t-on au sujet de l’intégration professionnelle des diplômés internationaux en médecine au Canada?. Healthcare policy = Politiques de sante, 12(4), 18–32. https://doi.org/10.12927/hcpol.2017.25101
Newton C. (2023). Family medicine has become more complex: New funding model is a welcome first step. Canadian family physician Medecin de famille canadien, 69(4), 295. https://doi.org/10.46747/cfp.6904295
Palmer, K. S., Martin, D., & Guyatt, G. (2013). Prelude to a systematic review of activity-based funding of hospitals: potential effects on cost, quality, access, efficiency, and equity. Open medicine : a peer-reviewed, independent, open-access journal, 7(4), e94–e97.
Pinsky, M.R., Bedoya, A., Bihorac, A. et al. Use of artificial intelligence in critical care: opportunities and obstacles. Crit Care 28, 113 (2024). https://doi.org/10.1186/s13054-024-04860-z
Sarabdeen, J., Chikhaoui, E., & Mohamed Ishak, M. M. (2022). Creating standards for Canadian health data protection during health emergency – An analysis of privacy regulations and laws. Heliyon, 8(5), e09458. https://doi.org/10.1016/j.heliyon.2022.e09458
Yangzom, K., Masoud, H., & Hahmann, T. (2023). Primary health care access among First Nations people living off-reserve, Métis and Inuit, 2017 to 2020 (Catalogue No. 41-20-0002). Statistics Canada. https://www150.statcan.gc.ca/n1/en/pub/41-20-0002/412000022023005-eng.pdf
Featured Image: Adobe Stock
Appendix